 Print This Post
Print This PostIn this post I will discussing Public Patient Involvement, unpacking what that actually means in respect of other similar concepts such as participation and engagement, how PPI can be done throughout the research process, and drawing on my experiences of intentionally and unintentionally doing involvement activities. If you are just starting out with you studies this could be helpful to support PPI elements in your research proposal and ethics, or if your research is underway like me, it may just be useful to validate your activities and situate them in the research process.
If you’re interested or involved in dementia research you will be well aware of Public Patient Involvement [PPI]. PPI recognises that people’s views may differ from those of professionals and researchers and much research supports this. Therefore it is about being more accountable and transparent to the people and communities we are trying to serve by “doing research with or by the public, rather than to, about, or for them” (INVOLVE, 2012). It’s easy to see the commonalities between the underlying values of PPI and the desire for dementia care and support to enable and empower citizenship. Considering the morally just basis and emerging evidence base that supports PPI as a mechanism for improved health research ethics, impact, relevance, and cost-effectiveness, it is unsurprising that there is national and international belief that people should be at the heart of decision-making. Although how this looks in practice is not always black and white.
If I’ve engaged have I involved? And if I’ve consulted then have I collaborated?

Nathan demonstrating PPI in action.
Despite being a relatively new field of thought and practice, there is much, much, and much more to read in the area, however perhaps the biblical base for PPI is INVOLVE, the UK’s leading public participation charity, principally operating to involve the public in decisions that affect their lives. However public involvement can sometimes find itself misrepresented in other research activities. INVOLVE guidance for health researchers distinguishes three activities where involvement can become a little ambiguous and overlapping with other different, but similar, research activity, such as participation and engagement.
Participation is described as “people taking part in a research study”, engagement “where information and knowledge about research is provided and disseminated”, and involvement “where members of the public are actively involved in research projects and in research organisations”. By definition these may sound different activities but in reality the relationship is far less distinct. For example in my research I interviewed people and a discussion was had regarding the purpose of the evaluation: internal development or external funding? Therefore enabling people through participation to ‘identify research priorities’, i.e. be involved. I would add that involving people in the research isn’t always a formal strategic action. I’ve had a kick about, baked bread, drank tea and ate many a biscuit, while simultaneously engaging with people in discussions that have had significance to the research process.
The approaches of PPI, ‘consultation’, ‘collaboration’, and ‘user-controlled research’, are similarly entangled concepts. Consultation is when you gain public view and use this to inform decisions about the research; consultation is when you formally discuss aspects of the research process for example the methods of data collection or dissemination routes; and user-controlled research is research actively “controlled, directed and managed” by people and organisations (INVOLVE, 2012), akin to coproduction methods and the great research being led by people affected by dementia.
Again, as with engagement and participation, naturally, consultation is a collaborative activity, where, in the case of my research, I have asked people to identify research priorities (consultation) and if I may consult with them again about the outcomes I believe are emerging form the initial stages of data collection and how best we can measure these (consultation again), so that key research decisions are shared (collaboration). I will then consult with stakeholders once more on the findings of the research and how best to disseminate these in a way which (1) represents the varying audiences voices present in the study; and (2) is the best method for embedding results to improve practice (consultation and collaboration).
Dr Kath Maguire and available at https://www.gu.se/en/gpcc/patient-and-public-involvement-ppi-in-research-how-when-and-why
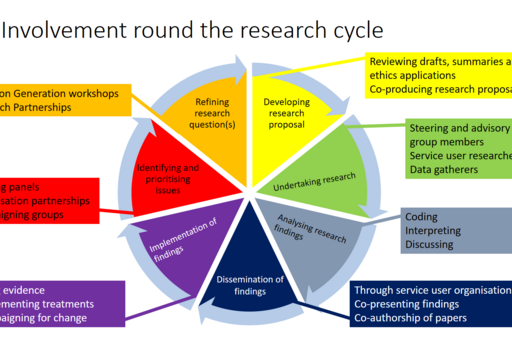
While I am clearly arguing the process, activities, and approaches of PPI (encompassing engagement and participation) should not be dichotomised, I do find visual representations of how people can be involved useful to situate my projects PPI elements in precise slices of the research process.
What I would add as a closing thought and reflection on my experiences of PPI to date, is that the how and why for doing, or not doing PPI should be well deliberated. At the start of my PhD I was naïve to look at what experienced researchers were doing and think that’s it, I’ll do that! Over ambitiously referencing National Reference Groups, DEEP, and TIDE while not taking into full consideration the broader research project and process: the research study context, population and aims and objectives. But I have now come to learn it’s good practice during a PhD to reaffirm exactly what it is – a training course to become a competent and confident researcher – so I try to take a proportionate approach in terms of what I want to do, what is necessary, and what is doable, while making sure the underpinning principles of public involvement, including accountability, transparency, and democratic justice, remain present.
Nathan
-
Miah, J., Dawes, P., Edwards, S., Leroi, I., Starling, B., & Parsons, S. (2019). Patient and public involvement in dementia research in the European Union: A scoping review. BMC Geriatrics, 19(1), 1–20. https://doi.org/10.1186/S12877-019-1217-9/TABLES/4
-
Health Research Authority / INVOLVE (2016), Impact of public involvement on ethical aspects of research. www.invo.org.uk/posttypepublication/public-involvement-in-researchimpact-on-ethical-aspects-ofresearch
-
INVOLVE. (2012). Briefing notes for researchers: public involvement in NHS, public health and social care research. https://www.invo.org.uk/wp-content/uploads/2012/04/INVOLVEBriefingNotesApr2012.pdf

Nathan Stephens
Author
Nathan Stephens is a PhD Student and unpaid carer, working on his PhD at University of Worcester, studying the Worcestershire Meeting Centres Community Support Programme. Inspired by caring for both grandparents and personal experience of dementia, Nathan has gone from a BSc in Sports & Physical Education, an MSc in Public Health, and now working on his PhD.



I have dementia, and am a researcher in my own right. I respectfully must disagree with you; we cannot be involved enough. We know what needs to be researched, and can give invaluable lived experience.
Hello and thanks for commenting, its nice to get some feedback and know the posts are reaching people.
I am sorry if I have not presented my views well in the post well. Just to be straight, for me, involving people affected by dementia in research and policymaking is central for the points you make and many more.
I would be interested to know where I have misrepresented my views? MY research has a very strong stakeholder involvement approach and if I can make this point more clearly that would be great for me to know.
Many thanks, Nathan.